Introduction
Mid-2021, when happily leveraging my company's sponsored annual full-health check-ups, one of my visits ended in awkwardness when the doctor said "your heart sounds funny", along with some ominous pronouncements about the impossibility of any new medical insurance. Innumerable cardiologist conversations later, it culminated in an eventual open-heart surgery conducted at Mount Sinai in New York City, even though up till the surgery I was essentially asymptomatic.
I wanted to spend some time to go through the journey, in case it helps better inform anyone about their own journeys through similar troubles; and perhaps give myself a bit of a retroactive look at my journey many years on.
The Diagnosis
It began with a regular health check-up electrocardiogram in 2021; the cardiologist looked at it, noticed oddness, then chose to listen to my heart and noted a 'murmur'. A followup 2D-echocardiogram confirmed that the likely cause was Bicuspid Aortic Valve Disease, with the 'wooshing' sound of my heart caused by the aortic regurgitation that was occurring with every pump.
It's pretty hard to get definitive imagery for bicuspid valves, which are deeply nested within the body. The standard practice today is to use echocardiograms, which are essentially ultrasounds pointed at the heart. 2D echocardiograms give us 2D 'cross-sections' of the heart, at a depth defined by the tool's controls; watching this cross-section over time allows one to see the movement of the valve over the plane, and hence approximate the rough structure of said valve. Here's a quick GIF of one of my 2D echoes from 2021:

What is BAVD?
This is a gist gathered over my conversations with doctors, my research, and conversations with various LLMs. In a nutshell:
- Bicuspid Aortic Valve Disease is a congenital condition where instead of the typical three-leaflet setup in my aortic valve ("tricuspid"), there are only two leaflets in mine
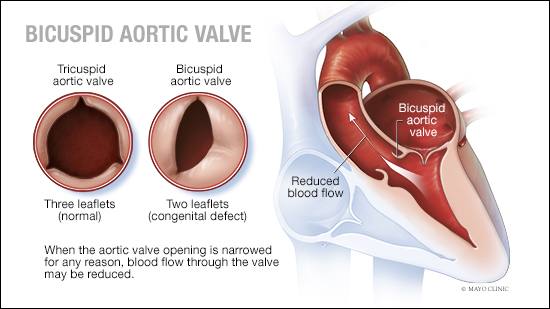
- This leads to nontrivial amounts of aortic regurgitation during 'diastole', when the heart is relaxed - some blood flows back through the improperly sealed aortic valve, which can have several physiological downstream impacts:
- The blood flow can lead to the left ventricle enlarging over time ("LV dilation/remodeling"), as it deals with increased volumes of blood per pump (new blood + unnecessarily regurgitated blood).
- If the jet is eccentric (as mine was), it can cause micro-lesions within the heart.
- Untreated, this can manifest in "shortness of breath, difficulty exercising, lightheadedness or chest pain", culminating in possible heart failure after years of accumulated wear.
Markers and follow-ups
With a bicuspid valve, there's no medicinal solution given that it's a structural issue with the heart; the only fixes possible are physical repair or replacements of the valve. According to my doctors, the aortic valve in particular is difficult to replace via catheter; per the cardiologists' recommendations, the only recourse is to perform open heart surgery (!!) to gain physical access to the valve itself.
Open heart surgery is obviously one of the most drastic actions one can take; it's as 'invasive' as it gets for a surgery. Notwithstanding the severity of the surgery, the remedies themselves are not cure-all fixes. The options, as laid out by my Singaporean doctors, were both of replacing the valve entirely, with either of:
- A biological valve (usually a pig valve).
- Biological valves were outright disqualified for me, as they tend to have durabilities of 7 to 15 years, especially in younger patients; given my age, the combination of this with the need for 'frequent' reinterventions (each subsequent surgery introduces higher risk) made it infeasible.
- A mechanical valve, which would require me to take blood thinners (warfarin) for the rest of my life.
- Mechanical valves have a series of risks as well, with possible infections, strokes, and complications with blood thinners making it essentially a lifelong-managed condition, with still impacted reductions in life expectancy and quality-of-life.
Given the drastic downsides of both options, cardiologists tend to advocate the delaying of conducting surgery as long as possible. They generally use thresholds on a few markers to guide their decision on whether or not to intervene:
- Ejection fraction: The estimated percentage of blood being successfully pumped with each contraction of the heart
- Left ventricular diameter exceeding a certain threshold
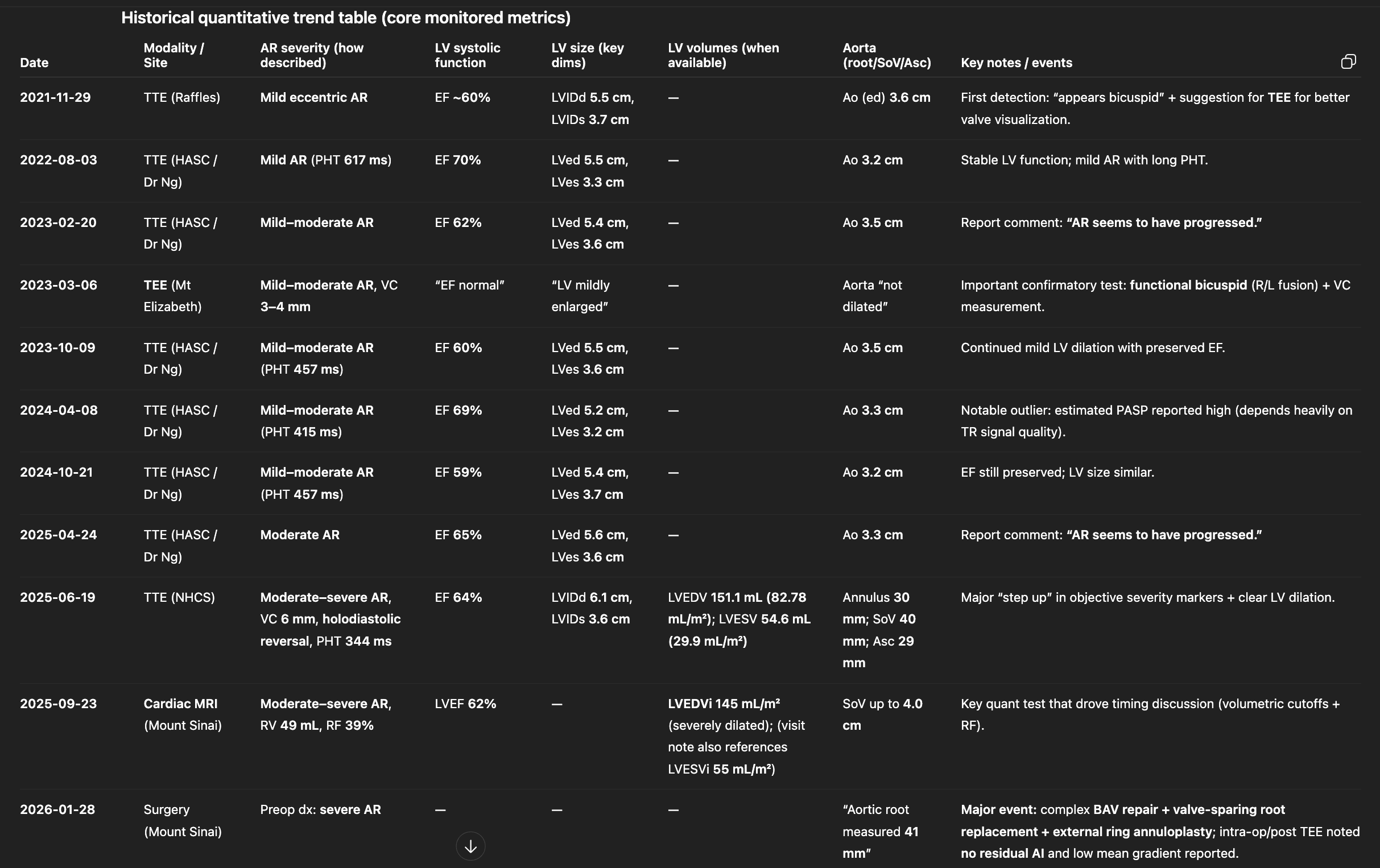
Given that my estimated regurgitation was 'mild-moderate' at the time of discovery (2021) and only progressing to 'moderate' up through 2024, I was content to manage the condition via periodic (6-month) followups with my cardiologist.
Escalation
Unfortunately, there seemed to be notable progression in the rate of my regurgitation, having progressed from 'mild-moderate' in 2021 through to 'moderate' in late 2024 and 'moderate-severe' in 2025. I'd consulted four different cardiologists in Singapore at this point, with the general consensus still being to delay as much as possible, given my EF and LV diameters still remaining within reasonable thresholds.
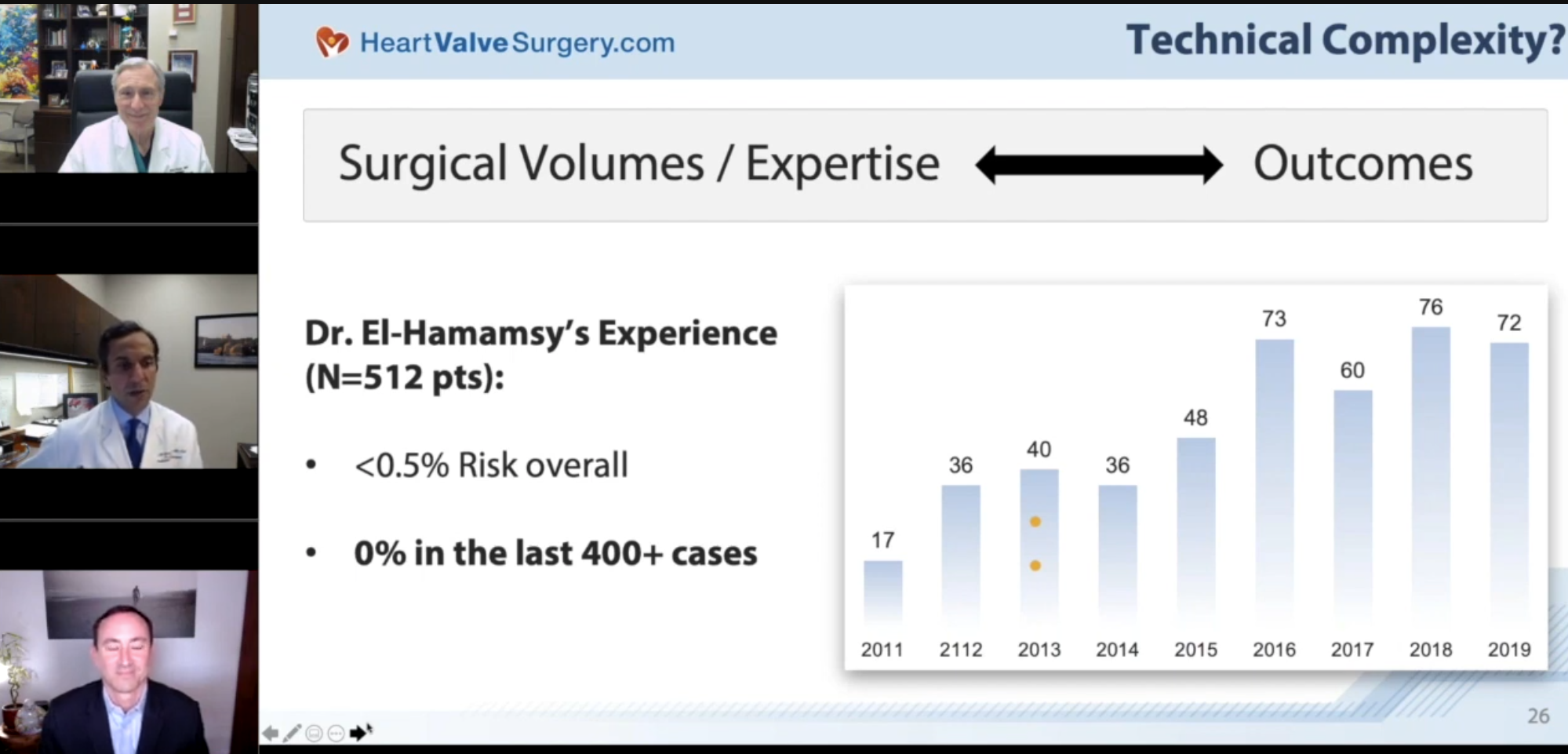
On the side, though, I was watching other online sources (notably, r/valvereplacement) on how others were handling similar conditions. This turned out to be influential. Some surgeons' names frequently surfaced as being world-renowned for their experience, with some centers being reputed for their high volume of treatments of similar conditions. This, along with a fortuitously timed work trip to New York City in September 2025, led to me scheduling a consult with Dr Ismail El-Hamamsy of Mount Sinai (from the video above!).
The initial consult was very informative; he has dealt with many patients of my age and profile, and ultimately his perspective was similar (delay as long as possible, watch markers for thresholds). However, the measure he used differed from that of my Singaporean cardiologists; he preferred to use Left Ventricular Volume (normalized), rather than the diameter. This is harder to track, as this requires an MRI rather than a 2D echo (to give a bit of a benchmark; MRIs cost ~3-5x more in Singapore). He also offered an additional set of operative alternatives to the valve replacements: Aortic valve repair, and the Ross procedure:
- Aortic valve repair involves reshaping the existing valve leaflets and reinforcing the aortic root with synthetic grafts and a stabilizing ring. He estimated that statistically the durability of this would last about 20-25 years.
- The viability of this is subject to conditions he can only tell during the surgery itself; it involves feeling the pliability of the valve, suitability of the existing leaflets, etc.
- The Ross procedure involves replacing the aortic valve with the pulmonary valve, and replacing the pulmonary valve with that of a human cadaver's.
- This is one of the most 'complex' options given the multiple steps and components involved.
- Rough estimates of durability were about 15-20 years.
- Also not a given; highly subject to feasibility of the pulmonary valve as a substitute for the aortic valve.
- Notably - Dr El-Hamamsy is world-renowned for this procedure, with Mt. Sinai being one of the highest volume centers in the world.
Given the short-term nature of my visit, he sent me for an expedited MRI in Mt Sinai, which discovered that my left ventricular volume exceeded his thresholds by ~20%. In a hastily arranged subsequent MRI-review consult, he suggested that the best way to optimize for lifespan and an active lifestyle was to intervene within the next 6 months, to give the left ventricle the best chance to remodel.
All in all, his laid-out plan for me with the goal of me being able to "blow my 90th birthday candle" was:
- Repair of the valve, if possible (best case scenario)
- When the repair begins to fail OR the repair is deemed infeasible, conduct a Ross
- When the Ross fails OR the Ross is deemed infeasible, do a valve replacement with mechanical or biological valves (likely mechanical, given my age)
This would require leaving a fair amount of trust to his subjective intra-operative decision making; I'd be going into surgery without a clear idea of the eventual decision made. Of note, however, was his confidence in the operation; maybe because of his experience (he's done ~1300+ similar operations), he was very confident in the chance of success, with an estimated lethality risk of <0.5% (I don't know, this still seemed a little high to me, but I don't have a Bayesian anchor for this number...) and a reasonably high estimation that a repair was possible based on the existing imagery he had. This dispelled to some degree my instinctive apprehension over the 'severity' of an open heart surgery.
The Dilemma
This left me with a bit of a dilemma; Singaporean and American opinions significantly diverged on both my operative options as well as surgical timeline recommendations.
I had several followup appointments with cardiologists in Singapore; even a Ross specialist in Singapore (sadly, Singapore is a much smaller-volume center, but I felt it was good to get as many views as possible). The general consensus was:
- Doing a repair or a Ross in Singapore is highly unlikely.
- Repairs aren't a well-established solution (in Singapore, at least) - some deeper research revealed that aortic valve repair is a relatively modern innovation and it's likely that the state of affairs in Singapore just hasn't caught up yet.
- At a ~1-2% natural incidence rate of BAVD, combined with the largely asymptomatic nature for young patients, and our tiny population, odds are that they just don't see enough people with my condition.
- Ross procedures are typically only done here for the very young when there is no other choice (no viably-sized valve replacements for child hearts). Our volume for the Ross is more on the order of <10 per year, compared to Mt Sinai's hundreds.
- They commonly cited "you're turning a one-valve-disease into a two-valve disease"; this was addressed in the video above, whereby they cite that statistics are more important, and that the statistics for high volume centers for Ross outcomes are excellent (to be honest I would agree with this).
- Repairs aren't a well-established solution (in Singapore, at least) - some deeper research revealed that aortic valve repair is a relatively modern innovation and it's likely that the state of affairs in Singapore just hasn't caught up yet.
- Mt Sinai is a highly reputable center for heart surgeries; one even congratulated me and shook my hand (probably a little tongue-in-cheek?) - they know what they're talking about, and their recommendations have credibility behind them.
- The cost is exorbitant compared to one in Singapore; honestly it was only possible for me because of my extremely generous company insurance coverage.
- Their general recommendation is still to delay given that they are following existing established guidelines; but they acknowledge the experience/credibility of the alternative opinions.
| Location/Decision | Credibility | Risk | Lifestyle impact | Longevity | Cost |
|---|---|---|---|---|---|
| Singapore (Delay, mechanical valve) | 4 cardiologists consulted; following established ESC/ACC guidelines | Continued LV dilation while waiting; eventual mechanical valve carries lifelong warfarin risks | Lifelong blood thinners, dietary restrictions, bleeding management | Reduced life expectancy vs. general population | Relatively affordable (<S$20k presumably) |
| NYC (Operate now, Repair/Ross) | Dr El-Hamamsy, ~1300+ operations; Mt Sinai, one of the highest-volume centers globally | Surgical risk (<0.5% mortality); repair durability ~20-25 years | Near-normal lifestyle post-recovery; no blood thinners | Ross data suggests similar-to-general-population life expectancy | Exorbitant, but covered by corporate insurance for now |
I eventually decided to go ahead with Dr El-Hamamsy's recommendation, as:
- My regurgitation progressed relatively significantly in late 2024-2025 alone (mild-moderate -> moderate -> moderate-severe -> 'basically severe') over a series of 4 echos/MRIs, which is really concerning if we do a recency-biased linear extrapolation.
- My opportunity to do the operation in NYC is limited to the period during which I have generous healthcare coverage; nothing's to say this will remain true 10 years later.
- Ross procedure statistics have shown similar-to-general-population life expectancies
- Intuitively, I generally agreed with the instinct for preventative measures, to intervene while there is a good chance the heart can remodel to safe thresholds.
- Based on existing echocardiogram imagery, Dr El-Hamamsy was reasonably confident a repair was possible, and very confident in the success likelihood of the surgery.
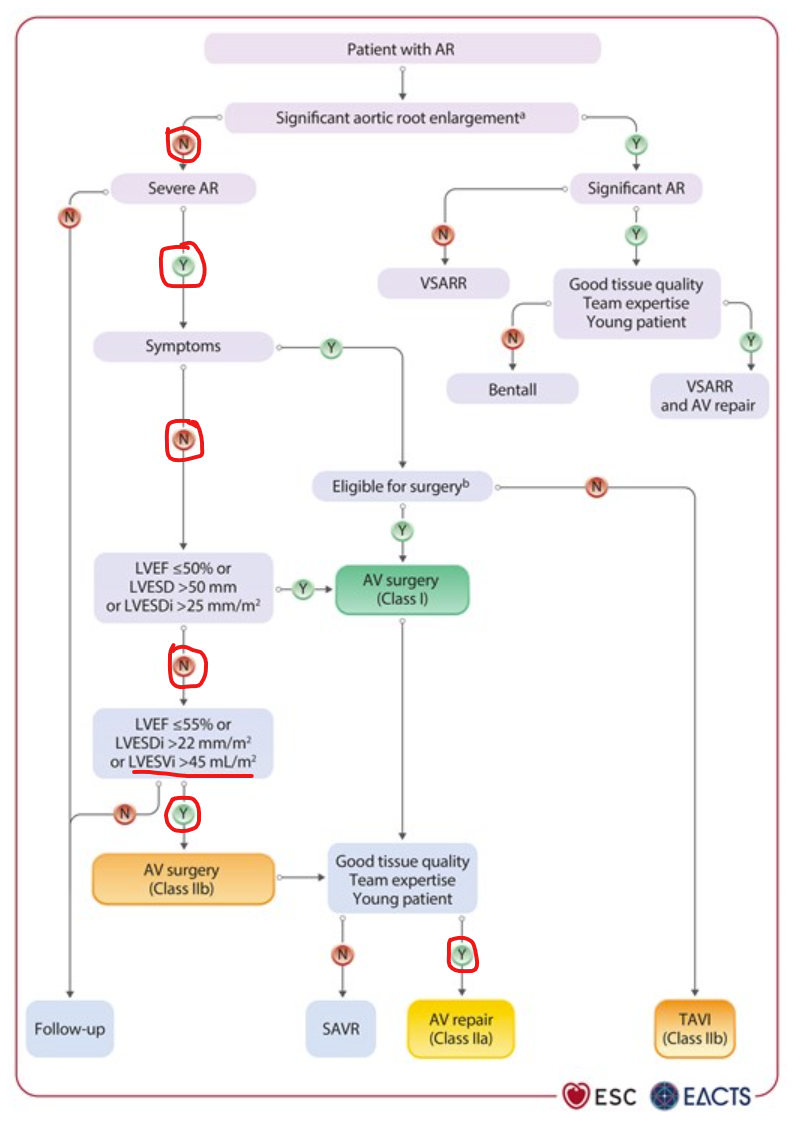
- His threshold and recommendations actually align with the 2025 ESC/EACTS Guidelines for the management of valvular heart disease:
- Small caveat - 'Class IIa' actually means it's elective (up to the patient's discretion), and hence not a strong recommendation, but the flowchart is an implicit endorsement nonetheless
The Surgery
Pre-operative checks
I flew into NYC on 24th January with my parents and partner, just in time for the coldest snowstorm in NYC in 10 years. We checked into a hotel selected mostly with distance-to-hospital and availability-of-a-gym in mind. We had a pre-consult with Dr El-Hamamsy and his team to get pre-clearance for surgery; there were prerequisites like blood tests, a chest X-Ray, screenings for Staphylococcus in my nose, and the like. It was also a good chance for my family to meet the surgeon who'd be operating on their son. I'd like to think this did plenty to help assuage their concerns as well; Dr El-Hamamsy even recommended that they go watch a show during the operation instead of worrying around outside (I'm glad they eventually followed his advice! They said MJ was pretty good, though (spoilers) they were interrupted halfway by his phone call indicating the surgery's success).
Surgery Day
We headed in at 8am and had a nice long brief on the procedure and forms; I had something like 5 different holes poked in me for various things like IVs (why did they need like 3 IVs?), blood tests, and so forth. After saying farewell to my family, they brought me to a 'general ward?' where different parts of the surgical team introduced themselves to me over time (several anaesthesiologists and nurses, as well as doctors on Dr El-Hamamsy's team). After about an hour of this (and some forms signed), they wheeled me into the operating room, which (to no surprise, I suppose) looked just like any other medical show's operating rooms, with blazingly bright lights and people decked out in scrubs behind complex-looking equipment.
General anaesthesia is really a work of modern magic; it's my second time having undergone this. I barely remember five minutes of being in the operating room itself, with the (very nice) anaesthesiologist conversing with me till unconsciousness. The next thing I knew, I was barely groggily awake, with a dull ache in my chest, and my girlfriend giving me news about my company's CTO leaving (?). Thought I was dreaming, but nope, that's just how life works. That, along with me insistently asking about the result of the surgery (remember - I had no idea of the eventual surgical option going into the op), is all I remember of the surgery and the immediate aftermath. I was told I had a breathing tube put in, but thankfully I only woke from the surgery after the tube was removed.
Happily for me, the surgery turned out to have gone very well; there were no unexpected hiccups, the repair was deemed feasible, and the operation completed in 3.5 hours, much faster than the usually expected 4-6 hours. It seemed the stars aligned, which is honestly as much as I could've asked for, and I say this with no small amount of gratefulness to Dr El-Hamamsy's excellent team :).

Recovery
The general timeline for the recovery from an open heart surgery tends to span three months, and my experience so far has tallied with that; going into details...
Hospitalization
Hospitalization started with one day in the ICU, and 4-6 days in a 'cardiac step-down ward' after. The staff were fantastic throughout, with good care and surprisingly good food; I quite enjoyed the hospitality of Mt Sinai's GP-7 West Cardiac step-down ward.
I emerged from the surgery with a few lingering... attachments? A chest tube, a pacemaker, a catheter, a 24/7-on HR monitor (for vitals alerting, I'd presume), and an IV drip. The chest tube was plugged directly into my chest (below the incision). That aside, there were a few major pains to recover from:
- My sternum, having been sawed open and stitched back together, had to fuse back together
- Everything damaged en route to my heart had to heal
- The chest tube was still actively draining blood + inflammatory fluids from the empty space around the heart ("mediastinal/pericardial" space), to prevent buildup during my recovery
- Everywhere I was poked with a needle (most notably my neck, for one of the IVs) also had to heal
- My lungs couldn't expand fully on account of all of the above chest damage
- Significantly reduced stamina on account of the above
Chronologically, my experiences:
Day 0
The evening of Day 0 was the worst, by far; though the operation itself completed early-afternoon, I only came to in the evening, flitting in and out of consciousness. My first memory is of feeling severe dehydration, frequently asking for water (and I'm told ice chips, though I don't remember this part).
- This unfortunately spectacularly backfired with several bouts of severe nausea, which is apparently a common side-effect of anaesthesia. This led to me vomiting or dry-heaving several times over the night, which felt like hell combined with the pain in my chest.
- I remember thinking this was one of the longest nights of my life, on account of the parched-ness, the dry-heaving, and the feeling of fear-of-drinking-for-fear-of-puking. I had a mini-anxiety attack at some stage, which was really strange as I've never had that 'impending sense of doom' feeling before.
- In the ICU, nurses were allocated to patients at a 1:1 ratio; I was really thankful for this, as I'm sure I was a handful over the entire night with my periodic struggles. The nurse was a constant reassuring presence, wiping me down and providing me consolations on how it would all blow over soon.
Day 1
Day 1 was a slow-burn of 5-6/10 pain; this was the first time in my life I noted the efficacy of painkillers on myself (I'd taken Panadols before, but more on doctor's advice rather than marked observation of effects on my body).
- Admittedly, the painkiller they administered was oxycodone, which is a strong opioid analgesic. No wonder I felt obvious relief from it. I promise I'll have no dependency though! They only gave me 14 days' worth, haha.
- I was also given an Incentive Spirometer and advised to train on it 5-10 times an hour. While the initial readings were somewhat discouraging, it really helped me keep a bead on my lung recovery progress. Day 0: 300mL
- The feeling of having a catheter attached is very interesting - throughout the entire period, I had no urges to pee at all, and liquid simply naturally dripped (or it was sucked?) its way into the catheter container.
Day 2
On Day 2 (I think?), the pacemaker, catheter, and the incision patch were removed, allowing me to see my incision for the first time; a mess of stitches and glue, that I was strongly advised to avoid disturbing. To avoid disturbing viewers too, I won't put a photo here :-)
- Day 2 is when I began trying to physically walk; my first time was with the help of a physical therapist, we did a round around the ward and I noted the very odd dichotomy of exhaustion in the chest while feeling perfectly fine in the legs.
- Walking around was pretty annoying, because you essentially need to carry around all the attached equipment with you while walking (chest tube fluid drainage tank, IVs if any, live HR monitor, and catheter drain tank). However, walking is apparently one of the best ways to speed up recovery (according to ChatGPT), so I tried to walk around the ward several times a day from this day onwards.
Day 3
On Day 3, the chest tube was removed (yay!). Online research implied this is usually the turning point of pain, though to be honest I didn't notice any major uptick in quality-of-life; the chest tube incision still hurt, though maybe got aggravated less from not having something shifting around whenever I moved.
Day 4
On Day 4, I was able to walk laps around the ward without much difficulty, and was down to an averaged-out 2-3/10 level of pain (rather bursty in nature). However, doctors noted some elevated liver enzyme numbers, so decided to hold me till day 5 before discharge.
- I had a bout of runny-nose induced coughs, which was really harsh on the chest, causing spikes of intense pain (and a desperate instinct to hold in my coughs). This went on to plague me over the next 10 days, surfacing on-and-off, notably correlated with physical fatigue and mild throat irritants (most memorably, Milo powder and Tiramisu powder...).
Day 5
Day 5: Discharge! Day 5 was also the first day I could shower myself, leaving me feeling clean and ready to move on.
Post-discharge (NYC)
Post-discharge, I was more or less ensconced in my hotel room in NYC (and the gym downstairs). Luckily, we had the foresight to upgrade to a suite room (so a living room + bedroom) with accessibility features, so a lot of accommodations worked out in our favor:
- Handholds in the bathroom for stability
- Ample space (suited for wheelchairs presumably)
- Pretty good temperature control
- Close proximity to the elevator
I was also instructed to keep track of several metrics over time:
- Blood pressure: Targeting systolic BP of <110 mmHg
- Temperature: Watching out for fevers
- Heart Rate
- Weight: Watching out for sudden weight gain (for fluid retention)
I was also given a medley of medicines to manage these, along with pain medication for lingering pains (which were generally ever-present).
Some thoughts on this period:
- I found it pretty hard to get continuous stretches of sleep, on account of the numerous aches across my chest; I found that there was no 'stable bed position' in which I could comfortably lie for over 3-4 hours, with whichever load-bearing part of the chest feeling increasingly sore over time.
- Sleeping on my back was basically a must up through Day 14; on Day 14, I found I could (periodically, for short bursts) lie on my side to ease the accumulated ache from lying on my back
- Sitting up from a lying position was really tough, given the constraints (no arm-lifting of anything >4 kg), especially because our hotel bed was too damn soft (normally a good thing...). Note to self, train up core-strength next time...
- My spirometer 'performance' grew; the doctor's given benchmark was 1000mL, and I was able to hit 2500mL by day 15, which was a massive improvement compared to the original shameful display of 300mL on Day 1.
We had a post-discharge review on day 13, during which doctors noted good recovery and generally good numbers on my blood tests, giving me clearance to fly back. A big factor in this was presumably my age; at age 30, it almost seemed like my concerns centered more around discomfort rather than overall ability to recover.
Helpful and unhelpful factors
What I found really helped in my recovery:
- A wedge pillow, which allowed me to 'sit up' for long periods of time with periodic angle and pillow-height adjustments. This also initially helped with sleeping, but by day ~10 I found the rigidity was starting to cause more discomfort than help so I started sleeping flat (with elevated pillows where possible).
- Lots and lots of UberEats (or loved-ones-taking-away-food) deliveries to cut on the exhausting journeys outside of the hotel in subzero temperatures
- Same for laundry - lucky me!
- Amazon - shopping distractions from pain aside, we could easily get lots of snacks and furniture/cutlery for our three-week stay off a one-month Prime membership. We even managed to get a refund for our (unused) shower chair!
- A lovely heart-pillow they gave me on Day 0 that accompanied me through my worst times; explicit instructions were to clutch it close to my chest during coughs to spread the impact across the entire chest rather than risk hurting the sternum's recovery. I suppose any chest-sized pillow would help here
- An easily accessible gym, where I began with staggered 15-minute walks and ended with regular 30+ minute 'faster-but-not-brisk-yet' walks near the end
- This tended to correlate with uncomfortable evenings of runny noses/coughing struggles, though, so sadly I wasn't as dedicated to these as I'd initially wanted
- Claude Max and Codex Pro subscriptions kept my mind occupied, rewriting my personal website and entirely vibe-coding a play-idea I was inspired by, which was to have my own personal butler.
- Learning the current SOTA of agentic development, and using the latest models (Opus 4.6/Codex 5.3) led me to believe models have just surpassed a cliff of usability for software engineering purposes; more to follow in other blog posts...
- I had to upgrade my Codex subscription after I blew past Claude Max's weekly limit after going a bit too far with subagents...
- A weighing scale, Blood Pressure monitor, and thermometer (I'd brought the latter two; we had to buy the weighing scale)
Not so helpful was...
- A shower chair, which others had suggested online; we had bought one, but it turned out that I could shower myself just fine from Day 5, so we ended up never using it. Probably much more helpful for older patients, who struggle with dexterity or with remaining standing while showering?
- Ibuprofen, which might have had some effect but really paled in comparison to oxycodone (after the oxycodone prescription ended). I wound up generally taking this every night in the (sometimes validated) hope that it would stymie my pain enough to give me a full night of sleep.
- I was advised against taking Paracetamol as my liver numbers were still slightly elevated, so no ideas on the efficacy there
- My second (portable) monitor which I'd brought hoping to set up a workstation; the desk setup wasn't optimal, and moving my neck turned out to be a little more uncomfortable than necessary
Managing Fatigue
I found through this experience that my body's reaction to fatigue is very disconnected from my mental sense of fatigue; when exerting, I'd mentally be feeling fine, but my body would be accumulating symptoms that would culminate in me having trouble sleeping. General progrssion:
- At the start of the hospital stay, my energy levels were pretty low; walking one lap around the ward was doable, but very uncomfortable.
- Near the end of the hospital stay 4-5 days later, I could do several rounds around the ward and a few flights of stairs without much trouble.
- Initial days in the hotel room were mostly centered around managing pain and discomfort; identifying comfortable sitting postures, sleeping strategies, etc.
- Mental fatigue being disconnected from physical fatigue was great for me as a programmer; I could simply throw myself into physically-unexhaustive projects! Like rewriting this website :-) and I would be very much distracted from the pains of recovery for hours at a time, interleaving Claude Code with bouts of sleep.
- Near the end of my stay in NYC (~Day 16), I was feeling energetic enough to go out for 1-2 hour lunches at nearby restaurants, and even had a 4-hour dinner/dessert with my girlfriend's cousin and his wife.
It was quite surprising to me that, coughing aside, there weren't any instances of excruciating pain throughout my recovery. All the pain felt was gradual and rather 'blunt' in nature, meaning they could be well-targeted with painkillers and, more importantly, distracted from easily with things like shows or programming. The main thing the pain impacted was sleep, as mentioned above, but I was pretty grateful that all of these problems were discomforts rather than complications during my recovery.
Flight back to Singapore
Luckily for me, my loved ones accompanied me on this trip; as a result, we didn't have to risk my interaction with heavy weights (luggage, carry-ons, etc.) as they helped to shoulder my burden. I'd underestimated the benefit of this; having had the feeling of chest pain with the incision interacting with simple daily tasks (like lifting a bowl of soup with outstretched arms), I could really tell that heavy weights were a no-go for my condition.
The flight itself was relatively uneventful, as I'd gone out on a limb and bought business class tickets for myself and my family (unironically, the largest expense I've ever spent in my life). I can't say I regret it; an economy-class seat for 18 hours with my wound would have been... survivable, but truly uncomfortable given the impact of posture on the pain. I spent most of it fighting with tailscale-vscode-remote-ssh on airplane wifi; during which I managed to write the vast majority of this blog post.
Going forward
Dental Health
Funnily enough, dental health is one of the major concerns going forward for the rest of my life. Infective endocarditis is a possible downstream complication with bicuspid valves and repairs/replacements. Antibiotic prophylaxis and daily flossing are now constantly in the back of my mind whenever it comes to worrying about my teeth.
Subsequent Ross/Valve
I now have an impending spectre of a potential valve replacement, hopefully more than 20 years down the line. This will be managed with annual 2D echocardiograms in Singapore to track LV size and regurgitation; I'm holding out some small hope that technological innovations grow in the interim to give me more surgical options, and also that we get even more data on the Ross such that it becomes a more globally standardized and accepted form of treatment for my condition.
Ultimately, I've accepted (or well, have accepted from the start) that there's no cure-all solution, and that the most important step to take is always simply the next step: Ask what is the best course of action to take now, given the information I know, the data I have, and the advice I've received. Many have wondered why my attitude towards the impending surgery almost seemed blasé; that's really because I was fairly confident that, at any point of time during my management of my condition, I'd already done everything I could and already received world-class advice on steps to take. Why worry, when there's nothing more to do? I suppose it's part of the philosophy of my life - no regrets and no fears, as long as all options have been explored and we've made the best possible decision :).
To anyone who might be reading this in a similar situation, I hope this was informative and helpful in some way; and to anyone who might be reading this in the future, I hope this was an interesting read, albeit being somewhat divergent in a blog that's normally about technical and geeky things!